Questões de Vestibular
Foram encontradas 68.627 questões
Resolva questões gratuitamente!
Junte-se a mais de 4 milhões de concurseiros!
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798992
Inglês
Texto associado

Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
De acordo com o quarto parágrafo, a profissão médica contribui para que as pessoas recorram à internet em vez de
recorrer a médicos. A justificativa apresentada é que
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798991
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No trecho do quarto parágrafo “the information we do like is
most credible, regardless of its source”, a expressão sublinhada equivale, em português, a
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798990
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No terceiro parágrafo, o termo “expertise” está entre aspas
para
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798989
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No trecho do primeiro parágrafo “I’d recommended that she
try a medicine”, o termo sublinhado pode ser corretamente
substituído por
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798988
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No trecho do primeiro parágrafo “Let me do some research
and I’ll get back to you”, o termo sublinhado refere-se
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798987
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
Em seu texto, a autora
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798986
Geografia
Analise um trecho da canção “As caravanas”, composta por
Chico Buarque.
É um dia de real grandeza, tudo azul [...] Quando pinta em Copacabana [...]
A caravana do Irajá, o comboio da Penha. Não há barreira que retenha esses estranhos Suburbanos tipo muçulmanos do Jacarezinho [...]
Com negros torsos nus deixam em polvorosa A gente ordeira e virtuosa que apela Pra polícia despachar de volta O populacho pra favela Ou pra Benguela, ou pra Guiné. [...]
(Chico Buarque. “As caravanas”. Caravanas, 2017.)
Nessa letra, o compositor
É um dia de real grandeza, tudo azul [...] Quando pinta em Copacabana [...]
A caravana do Irajá, o comboio da Penha. Não há barreira que retenha esses estranhos Suburbanos tipo muçulmanos do Jacarezinho [...]
Com negros torsos nus deixam em polvorosa A gente ordeira e virtuosa que apela Pra polícia despachar de volta O populacho pra favela Ou pra Benguela, ou pra Guiné. [...]
(Chico Buarque. “As caravanas”. Caravanas, 2017.)
Nessa letra, o compositor
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798985
Conhecimentos Gerais
A nova “autonomia” da juventude como uma camada social
separada foi simbolizada por um fenômeno que, nessa escala,
provavelmente não teve paralelo desde a era romântica do
início do século XIX: o herói cuja vida e juventude acabavam
juntas. Essa figura foi comum no que se tornou a expressão
cultural característica da juventude – o rock. Buddy Holly, Janis
Joplin, Brian Jones, membro dos Rolling Stones, Jimi Hendrix
e várias outras divindades populares caíram vítimas de um
estilo de vida fadado à morte precoce.
(Eric J. Hobsbawm. Era dos extremos, 1995. Adaptado.)
O autor descreve um fenômeno histórico que
(Eric J. Hobsbawm. Era dos extremos, 1995. Adaptado.)
O autor descreve um fenômeno histórico que
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798984
História
A chegada de Adolf Hitler ao poder, em 30 de janeiro de
1933, é celebrada pelos nazistas como a aurora de uma nova
era revolucionária. Imprensa, rádio e cinema são mobilizados
para convencer o mundo de que o povo alemão inteiro ajusta
o passo ao guia que ele escolheu. Manifestações grandiosas
tendem a provar que, num mundo dividido por lutas econômicas e sociais, a Alemanha hitlerista fundou a sociedade unanimista, com a qual muitos europeus fora da Alemanha sonham.
(Henri Burgelin. “O sucesso da propaganda nazista”. In: A Alemanha de Hitler, 1991. Adaptado.)
O texto apresenta o nazismo vitorioso na Alemanha como
(Henri Burgelin. “O sucesso da propaganda nazista”. In: A Alemanha de Hitler, 1991. Adaptado.)
O texto apresenta o nazismo vitorioso na Alemanha como
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798983
História
Na primeira República brasileira (1889-1930) associaram-se
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798982
História e Geografia de Estados e Municípios
O Rio de Janeiro, com seus 522 mil habitantes em 1890,
constituía o único grande centro urbano. São Paulo tinha 65
mil habitantes. Mas a cidade começara uma arrancada de
longo alcance, crescendo a uma taxa geométrica anual de
3%, entre 1872 e 1886, e de 8% entre 1886 e 1890.
(Boris Fausto. História do Brasil, 2012.)
O aumento demográfico de São Paulo no período mencionado no texto é resultado
(Boris Fausto. História do Brasil, 2012.)
O aumento demográfico de São Paulo no período mencionado no texto é resultado
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798981
História
Em toda essa diversidade de aperfeiçoamentos tecnológicos, era evidente o caráter unívoco do movimento: a mudança
gerava mudança. A oferta barata de carvão revelou-se uma
dádiva dos céus para a indústria do ferro, que estava sendo
asfixiada pela falta de combustível. Nesse meio tempo, a
invenção e a difusão de motores a vapor na indústria têxtil
criou uma nova procura de combustível, e, portanto, de carvão; e esses motores tinham um apetite voraz de ferro, o que
reclamava mais carvão.
(David S. Landes. Prometeu desacorrentado, 1994. Adaptado.)
O historiador refere-se à primeira Revolução Industrial, destacando
(David S. Landes. Prometeu desacorrentado, 1994. Adaptado.)
O historiador refere-se à primeira Revolução Industrial, destacando
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798980
História
Texto associado
Leia o texto para responder à questão.
O mundo procurado por Colombo mostrava-se esquivo.
Mas outro o aguardava, um mundo de riqueza mais fácil de
explorar. Na Mesoamérica e na região andina, nas terras habitadas pelos povos conhecidos como astecas e incas e em
suas imediações, havia redutos de densos assentamentos e
vida urbana, com os quais não se tinha contato. A incorporação
do continente americano levaria a Europa a deixar de ser uma
região pobre e marginal para se transformar num viveiro de
hegemonias globais potenciais.
(Felipe Fernández-Armesto. 1492: o ano em que
o mundo começou, 2017. Adaptado.)
A conquista espanhola dos “redutos de densos assentamentos e vida urbana”, ocorrida no início do século XVI, foi favorecida pelo fato de os incas e astecas
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798979
História
Texto associado
Leia o texto para responder à questão.
O mundo procurado por Colombo mostrava-se esquivo.
Mas outro o aguardava, um mundo de riqueza mais fácil de
explorar. Na Mesoamérica e na região andina, nas terras habitadas pelos povos conhecidos como astecas e incas e em
suas imediações, havia redutos de densos assentamentos e
vida urbana, com os quais não se tinha contato. A incorporação
do continente americano levaria a Europa a deixar de ser uma
região pobre e marginal para se transformar num viveiro de
hegemonias globais potenciais.
(Felipe Fernández-Armesto. 1492: o ano em que
o mundo começou, 2017. Adaptado.)
O autor sustenta que um mundo inesperado aguardava a
expedição de Cristóvão Colombo, devido
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798978
História
Por volta do ano 1000, consolidou-se no Ocidente uma
profunda mutação política e social. As antigas estruturas
públicas herdadas da Antiguidade terminaram por desmoronar para dar lugar a um novo regime, o feudalismo. Este não
é desordem, mas uma tentativa de instaurar uma nova ordem
fundada sobre as relações de homem a homem e sobre a
adaptação do poder a uma escala territorial reduzida, organizada em torno de um castelo.
(Jacques Le Goff e Jean-Claude Schmitt (orgs.). Dicionário analítico do Ocidente medieval, vol. I, 2017. Adaptado.)
Pode-se exemplificar a afirmação do texto com
(Jacques Le Goff e Jean-Claude Schmitt (orgs.). Dicionário analítico do Ocidente medieval, vol. I, 2017. Adaptado.)
Pode-se exemplificar a afirmação do texto com
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798977
História
A pirâmide de Quéfren e o obelisco de Luxor são dois monumentos do Egito Antigo datados, respectivamente, dos séculos XXVI e XIII a.C.
(www.pimpmytrip.it)

(www.molon.de)
Apesar das diferenças visíveis existentes entre esses monumentos, ambos exprimem
(www.pimpmytrip.it)
(www.molon.de)
Apesar das diferenças visíveis existentes entre esses monumentos, ambos exprimem
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798976
Geografia
Analise a representação das curvas de nível.
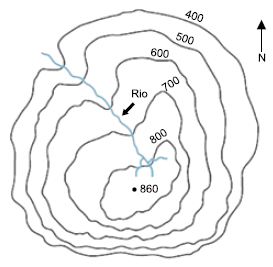
(https://glencoe.mheducation.com. Adaptado.)
Com base nas informações apresentadas, conclui-se que
(https://glencoe.mheducation.com. Adaptado.)
Com base nas informações apresentadas, conclui-se que
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798975
Geografia
Um grupo internacional de especialistas alerta que, caso
não sejam adotadas medidas mais drásticas para reduzir a
emissão de gases do efeito estufa do que as estabelecidas
no âmbito do Acordo de Paris, o teto considerado seguro para
o aquecimento global – de 2 °C acima dos níveis pré-industriais até o final do século – pode ser alcançado já em 2050.
(https://agencia.fapesp.br)
Entre os desafios para o cumprimento das metas do Acordo de Paris, pode-se mencionar
(https://agencia.fapesp.br)
Entre os desafios para o cumprimento das metas do Acordo de Paris, pode-se mencionar
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798974
Geografia

(https://sosgis.com)
A bacia hidrográfica ilustrada na imagem apresenta como uma de suas características principais
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798973
Geografia
O cinturão orogênico do Atlântico estende-se desde a
parte oriental da região Nordeste até o sudeste do Estado
do Rio Grande do Sul. É uma faixa de grande complexidade
litológica e estrutural, prevalecendo rochas metamórficas
de diferentes tipos e idades, como gnaisses, migmatitos,
quartzitos, micaxistos, filitos, e, secundariamente, intrusivas,
como granitos e sienitos.
(Jurandyr L. S. Ross (org.). Geografia do Brasil, 2008.)
Uma feição geomorfológica do território brasileiro integrante da área descrita no excerto é
(Jurandyr L. S. Ross (org.). Geografia do Brasil, 2008.)
Uma feição geomorfológica do território brasileiro integrante da área descrita no excerto é